Incident Reports
and Root Cause Analyses
2002-2008:
What They Reveal About Suicides
View Adobe Acrobat Version | Download Adobe Acrobat Reader
June 2009
New York State
Office of Mental Health

Michael F. Hogan, PhD
Commissioner
Lloyd I. Sederer, MD
Chief Medical Officer
Jayne Van Bramer
Director, Office of Quality Management
Among the reviewable sentinel events defined by The Joint Commission (TJC) is the suicide of any individual receiving care, treatment and services in a setting staffed around-the-clock or within 72 hours of discharge from such a setting. Incident reports submitted to the Office of Mental Health (OMH) reveal that this particular type of sentinel event occurred 122 times between 2002 and 2008. To present this number in context, NYS inpatient mental health treatment facilities operate approximately 3,660,000 bed days each year. Thus, limiting sentinel event (SE) suicides to approximately 17 a year is indicative of the skilled work of the clinicians serving these individuals. This report uses OMH incident reports to present historical data and a discussion of factors hospitals identified in their root cause analyses that may have contributed to the suicides or areas that otherwise called for improved performance. Every one of the 122 suicides is a tragedy that requires us to acknowledge its high human cost in anguish and pain and take measures to prevent a similar recurrence.
Every suicide is a tragedy that requires us to acknowledge its high human cost in anguish and pain and take measures to prevent a similar recurrence.
It is our intention that this SE suicide report will present an occasion for hospitals to review their policies and practices to ensure they are taking all measures reasonably possible to prevent this grave tragedy.
The Broader Picture
The most current in-depth analyses of national suicide data cover the years 2004 and 2005. The National Center for Health Statistics reports that in 2005, 32,637 people committed suicide in the United States, i.e., 11 suicides for every 100,000 persons and one suicide every 17 minutes. Suicide ends the life of more persons each year than does homicide or AIDS and HIV-related disease. It is the fourth leading cause of death in persons 18-65 years of age. In New York State during 2005, 1,189 individuals ended their lives by suicide. This rate of 6.2 suicides per 100,000 persons ranked New York 49th among the 50 states. While the low rank is heartening, looked at from another perspective, one of every 27 suicides in the nation occurred in New York State.Information from Incident Reports
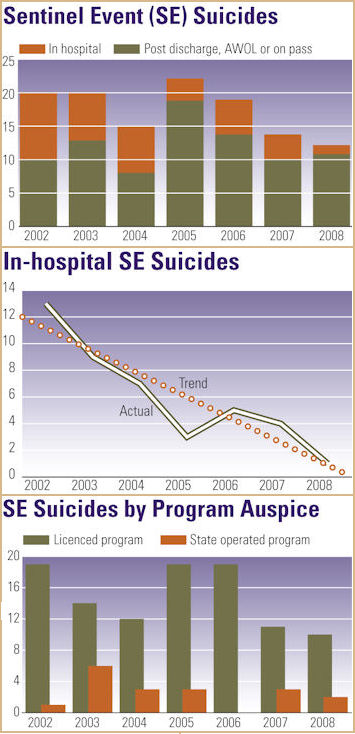
A review of the sentinel event suicides (inpatient or within 72 hours of discharge) reported to the OMH during the seven-year period 2002-2008 indicates that the yearly totals have fallen within the narrow range of 12-22. The most recent two years of the study period, 2007 and 2008, showed the smallest number of SE suicides. The location of the suicides-on inpatient units vs. post discharge or on pass/AWOL-has shifted. In recent years, post discharge suicides have significantly outnumbered in-hospital suicides. For purposes of this review, individuals who completed suicide while they were on pass from an inpatient psychiatric unit or if they had left the inpatient unit without permission are counted with individuals who completed suicide within three days of discharge. This allows us to look at factors affecting in-hospital suicides as distinct from those occurring in the community, beyond the supervision of hospital staff.
As illustrated at left, there has been a steadily declining trend in the number of in-hospital suicides between 2002 and 2008 which may be due, at least in part, to vigilance in identifying and correcting environmental suicide hazards, as reported by the impacted hospitals' Root Cause Analyses.
Suicides of persons recently discharged or on pass/AWOL have accounted for over half of the SE suicides each year, except for 2002. In the years 2005-2008, these suicides have represented 81 percent of the total study suicides as compared with 56 percent in the earlier three years. The American Association of Suicidology cites the month following discharge as highest risk, with most post discharge suicides occurring in the week following discharge.
Intuitively one might surmise that shorter lengths of hospital stays in recent years and increased reporting of post-discharge suicides have likely impacted the increase, but incident reports and root cause analyses indicate that systemic issues and the need to maintain clinical practice standards also factor in this increase as described later in the report.
A Closer Look at the Seven-Year Data
As would be expected, given the far greater number of persons served by licensed programs, in each of the years studied more SE suicides were reported by these programs, as presented below. This is true of both in-hospital and post discharge/on pass/AWOL suicides for the study period 2002-2007. In 2008, the single in-hospital suicide occurred in a state-operated facility. One in-hospital suicide occurred in an Article 31 hospital, in 2007.
Gender, Age and Race
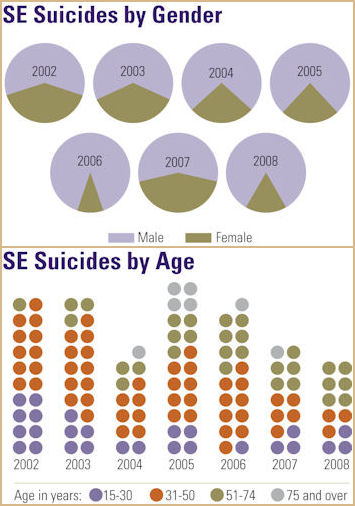
The National Institute of Mental Health (NIMH) reports that "almost four times as many males as females die by suicide."1 In four of the seven years studied, the OMH data reflected nearly the same or greater gender disparity than reported by NIMH. OMH incident data for SE suicides indicated that over the study period, the number of completed suicides involving women trended downward, despite the spike in 2007. At its highest, forty percent of the SE suicides were completed by women in 2002 and 11 percent, the lowest, in 2006. Of the persons who died from in-hospital suicides during the study period, 11 (30 percent) were women.
In contrast to the disproportionate number of men dying from suicide, no age group was spared, as evident in the wide age range among persons in the study group. Overall, these persons ranged in age from 15 to 93. Nearly half (48 percent) of the SE suicides were completed by persons aged 31-50. In 2002, 2003 and 2008 no persons 75 or older were reported as having died as a result of a sentinel event suicide. In contrast, the study group included one woman 93 years old who died by suicide in 2004, four persons in 2005 ranging in age from 75 to 85, an 87 year old man in 2006 and a 77 year-old man in 2007. At the opposite end of the age range, the youngest individuals in the study were a 15 year-old boy who hanged himself on an inpatient unit in 2007 and a 17-year-old young woman who also died in 2007 of self-induced asphyxiation while on pass from the hospital. The year 2002 was noteworthy because eight (40 percent) of the individuals who died from SE suicides were under age 30. Four of these young persons died on inpatient units-three by hanging and one by overdose. Two were on pass or AWOL; one dying by hanging and one from overdose. The remaining two individuals jumped to their death after discharge.
Of the 122 persons whose suicides were reviewed as sentinel events, 64 percent were identified as Caucasian, 10 percent as African-American and 11 percent as Hispanic. Asians constituted six percent of this group. In total, 27 percent of those studied were identified as persons of color. Consistent with data presented earlier, in all of the ethnic groups, suicides by males heavily outnumbered suicides by females. Caucasian males constituted the single largest category-57 percent of the total, followed by Caucasian females at 17 percent.
| Ethnicity | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | Total | Percent |
|---|---|---|---|---|---|---|---|---|---|
| Caucasian | 14 | 12 | 9 | 16 | 10 | 8 | 9 | 78 | 64 |
| African American | 2 | 3 | 2 | 2 | 2 | 1 | 0 | 12 | 10 |
| Hispanic | 1 | 3 | 2 | 3 | 3 | 1 | 1 | 14 | 11 |
| Asian | 2 | 1 | 0 | 0 | 1 | 2 | 1 | 7 | 6 |
| NA* | 1 | 1 | 2 | 1 | 3 | 2 | 1 | 11 | 9 |
| Total | 20 | 20 | 15 | 22 | 19 | 14 | 12 | 122 | 100 |
*NA=race information not available.
Suicide Method
Hanging and jumping from a height or in front of an oncoming vehicle were the most common methods of SE suicides in the seven years studied, as the table below indicates. The number of persons jumping to their death has increased as the number of recent discharge suicides has increased. Individuals who had been discharged within 72 hours or who were on pass or AWOL most commonly completed suicide by jumping from a height or in front of a subway or heavy motor vehicle. This method accounted for 40 percent of these 85 deaths. Death from gunshot wounds (13 percent) and drug overdose (15 percent)-in some instances street drugs, and in other instances prescription medications-were the next most common methods of suicide for this set of individuals.
| Method | Number | Percent |
|---|---|---|
| Hanging | 37 | 30 |
| Jumping | 36 | 30 |
| OD | 17 | 14 |
| Gun | 11 | 9 |
| Cutting/Stabbing | 6 | 5 |
| Asphyxiation | 4 | 3 |
| Drowning | 1 | 1 |
| Burns | 1 | 1 |
| Not Identified | 9 | 7 |
| Total | 122 | 100 |
| Location* | Number | Percent |
|---|---|---|
| Bathroom | 20 | 54 |
| Bedroom | 11 | 30 |
| Shower Room | 2 | 5 |
| Solarium | 1 | 3 |
| Hall | 1 | 3 |
| Office building | 1 | 3 |
| Not Identified | 1 | 3 |
| Total | 37 | 101 |
*in-hospital or under staff supervision suicides
Of the 37 suicides completed on psychiatric inpatient units or outside the hospital but under the direct supervision of hospital staff (one event), 28 (76 percent) were completed by hanging. From 2005 through 2008 all of the in-hospital suicides were by hanging. Most individuals who died by suicide on inpatient units ended their life by hanging themselves using their bedroom door or a door inside their bedroom-a closet door or more commonly a bathroom door. Grab bars in the bathroom, a closet door handle in the shower room, and the frame of a stretcher each figured in one in-hospital hanging suicide. Since the means are available and questions related to individual privacy often confound decisions regarding level of supervision and monitoring, these are not unexpected findings.
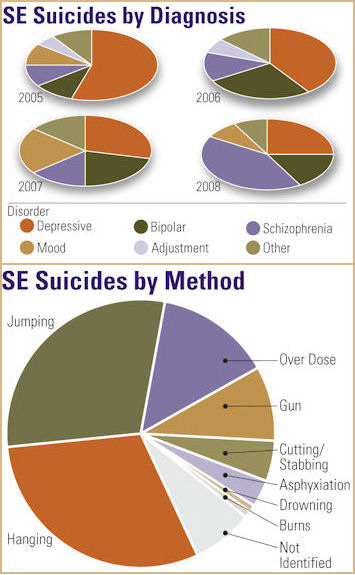
Methods of suicide over time are represented at right.
Diagnoses Diagnoses were available for 61 of the 67 persons who ended their life by SE event suicides in the years 2005 through 2008. (Data on diagnoses was not available for the earlier years of the study). In reporting diagnoses, the first-listed primary diagnosis was selected. The findings indicate that 67 percent of these individuals were diagnosed with a mood disorder. These figures align with those of the American Foundation for Suicide Prevention and the NIMH both of which estimate that 60 percent of persons who take their own life have a mood disorder. Persons with a diagnosis of schizophrenia (several types) made up 18 percent of the sample. Chronic pain syndrome, anxiety disorder, alcohol and polysubstance dependence and body dysmorphic disorder comprised the "other" category.
Suicide Root Cause Analyses:
Findings and Lessons
Root cause analyses of the SE suicides identified areas in need of improvement that included clearer and more frequent communication, including record documentation, by physicians and clinicians; staffing allocation and training; environmental modifications; and changes in policies and procedures. As if taken from a Joint Commission report that in 2005 identified deficiencies in communication and patient assessments as two of the most common contributors to inpatient suicides, root cause analyses of the sampled suicides most frequently identified the need to communicate effectively with families, other team members, and other treatment providers (and document that communication so that the information was available to all team members) and the importance of adopting or revising a suicide risk assessment tool.
Inpatient Suicides
With few exceptions, all of the root cause analyses completed after in-hospital suicides identified opportunities for improvement in the suicide/risk assessment process. These included the need to conduct and/or document a risk assessment, the use of more comprehensive suicide/risk assessment forms, and fully completed risk assessment process. Specific recommendations related to suicide risk assessments included:
- development of suicide risk assessment forms and training for psychiatrists and nursing staff in their use. The purpose was not to provide a checklist to be completed, but to prompt clinicians in their interviews to address all of the issues listed;
- enhancement of suicide risk assessments currently in use to discourage rote answers and ensure individualization. The risk assessment should address both dynamic and static risk factors. Static risk factors might include age, gender, history of impulsivity and previous suicide attempts. Dynamic risk factors might include a review of the crisis that precipitated the admission, the presence of current suicidal ideation and the availability of means and emerging stressors.2 For example, the decision by the individual's mother, with whom he had been living, to not allow him to return was not listed as a stressor in the assessment in question. In another instance, an individual working is this country on a work visa had recently lost his job. The treatment team needed to take these circumstances into account and the individual's stress at believing he may be deported.
- policy change to require that suicide risk assessments be completed on admission, again at 72 hours, and within 48 hours of discharge. The American Association of Suicidology (AAS) recommends that a risk-benefit analysis should be completed prior to decisions granting leaves, passes, and discharges for persons at high risk for suicide.
- modification to the suicide risk assessment to include a determination of risk level (low, moderate, high); and,
- expectation that suicide risk assessments will be completed daily for inpatients considered at high risk.
These recommendations reflect the current standard of care that would have a suicide risk assessment completed and repeated when clinically indicated, since the degree and intensity of suicidality is not constant. Clinical indications would include an abrupt change in clinical presentation and the lack of improvement or gradual worsening of condition despite treatment.3
Several hospitals identified the need for physicians to write orders when supervision levels of individuals were recommended for change. In some instances, the team had agreed to the increase in supervision, but no order was written and with inadequate communication, the enhanced supervision did not occur on all shifts. Another hospital revised its policies to require that all available team members assemble to reach a decision on supervision status. Still another hospital implemented an updated running log of persons on enhanced observation status kept in a prominent place in the nurses' station as a useful tool for staff to quickly identify individuals who need staff members assigned to observe them.
The absence of a comprehensive admission note that addressed past suicide attempts was noted as a factor in several inpatient suicides. Some clinicians spoke of their reluctance to speak about suicide in an interview, lest the topic agitate the individual or for fear of introducing the suggestion. Dr. Shawn Shea, a former director of a psychiatric emergency department, states in The Delicate Art of Eliciting Suicidal Ideation that in his experience errors in suicide assessments often did not seem to stem from poor clinical decisions, but rather from good clinical decisions based on bad data. The data most commonly absent or distorted "related to the extent of the patient's suicidal history, planning, and current intent."4
Some hospitals identified a breakdown in the process of securing prior records or in communicating with the referring program. Hospitals acknowledged that treatment teams had not reviewed earlier hospital records, even when they were readily available at their own hospital. In response, staff training and memos followed, clearly articulating the expectation that prior records be requested, secured and reviewed.
Several hospitals wrote procedures requiring the responsible staff member to contact mental health providers with whom an individual had had recent contact. This recommendation was repeated frequently, as hospitals, during the root cause analyses learned that staff had been operating with an inaccurate or incomplete picture of individuals' recent mental health status. This became particularly apparent when hospital staff learned too late that individuals had made previous suicide attempts. Several hospitals took other actions as well that included:
- instituting a checklist covering accessing historical records from all sources;
- developing a psychiatric transfer form to be used to document verbal communication between the sending and receiving psychiatrists;
- requiring the completion of a psychiatric history timeline for all individuals with four or more admissions. This timeline was to include information about diagnoses, medications, reasons for admission, and discharge arrangements; and,
- instituting structured interviews of family members to learn the family's and the individual's mental health history.
Many of the in-hospital suicide root cause analyses identified environmental issues that were either a factor in the suicide or were identified as potential suicide hazards. Corrective actions included:
- changing door hinges to piano hinges;
- removing all plastic bags from units;
- replacing drop ceilings so that the plumbing/ventilation above is not accessible;
- enclosing the plumbing under bathroom sinks;
- installing hallway mirrors;
- shortening television cables and nursing call button cables;
- locking tub rooms when not in use;
- removing hanger bars from wardrobes and closets;
- installing no-gap grab bars in showers, push button on/off shower valves, and shower heads that will not support a ligature;
- providing sturdier apparatus for securing air-conditioners;
- attaching emergency number stickers to all phones in patient care areas;
- mounting door-closing devices (V-shaped hinges a the top of the door) on the public rather than private side of the door;
- discontinuing the use of pajamas with ties or draw strings; and,
- using a weekly or semi-weekly Environmental Risk Assessment Tool.
Other improvements taken in response to in-hospital suicides, not surprisingly, included efforts to increase the effectiveness of monitoring rounds and other supervision measures. Many of these measures were accompanied by policy and staffing changes. Corrective actions included:
- increasing monitoring of the dorm area. Several hospitals identified varying the monitoring schedule so that rounds are staggered and less predictable.
- requiring that bedroom doors be kept ajar when individuals are resting;
- clarifying rounds procedures to include the requirements that staff observe an individual's movement during sleep, i.e., rise and fall of the chest, and have visual or verbal contact with the individual during daytime rounds;
- placing all newly admitted persons on every 15 minute monitoring
- for the first 24 hours;
- redesign of the physician coverage schedule and on-call procedures for weekends to increase coverage;
- assignment of specific staff members to monitor specific individuals who are on 15-minute checks;
- requiring staff to make verbal contact with and a response from individuals in the shower area during rounds;
- permitting the use of night lights or red-filter flashlights to facilitate nighttime checks;
- reduction in the unit census;
- implementation of semi-annual CPR drills to refresh staff's skills. In this instance staff panicked when they found the individual unresponsive and did not immediately initiate CPR.
- initiating a special paging code for life-threatening emergencies to differentiate these from general calls for assistance;
- revising visitor search procedures to prevent the introduction of contraband items, specifically, in this instance, drugs; and,
- revising 15 minute monitoring forms to require that the staff member document what the individual was doing, not simply that he/she was present.
In a particularly thoughtful root cause analysis, the hospital identified the need for training for staff to improve the quality of entries in the clinical record to reflect the uniqueness of the individual. It called for work on eliminating records that simply document the response to medications, daily routine, etc. and instead reflect time spent with the individual getting to know and understand him/her. Similarly, another hospital identified the need to challenge the "people-pleasing, everything is alright mask" worn by some individuals with suicidal intent.
Post Discharge Suicides
Lack of Effective Communication
Similar to concerns identified in reviewing in-hospital suicides, the importance of communicating effectively with or enlisting the assistance of family members was cited as an area requiring improvement in many of the post discharge suicides studied. Inadequate communication with the family or no communication at all resulted in a lack of information or erroneous information about the family's and individual's mental health history. This issue, together with the need to improve the content and use of a suicide assessment tool, were most frequently implicated in the suicides studied or were identified as areas that required improvement.
Several root cause analyses noted that the individual had denied the intent to harm him/herself and did not have a plan for self-harm. However, the clinician was not aware of the individual's passive suicide ideas and repeated iterations, such as, "I hope I don't wake up." Use of CASE (Chronological Assessment of Suicide Events) interviewing techniques might have elicited this information. In this interview, the clinician would explore in order suicidal ideation/attempts made within the past 48 hours, then within the preceding two months, past suicidal ideation/attempts, and any suicidal ideation occurring during the interview itself.5
In several instances, hospital staff did not make face-to-face contact with the family member with whom the individual would be residing at discharge. This resulted in insufficient exchange of information on such vital issues as:
- removal of guns from the home;
- the risks in mixing alcohol and psychotropic medication;
- the risks in taking prescription pain medication and psychotropic medication;
- increased suicide risk for persons who have attempted suicide in the past;
- the availability of contact crisis intervention services and how to contact the service; and,
- outpatient appointment information.
Grave consequences followed.
These deficiency findings led some hospitals to require that families sign a safety plan for the individual who was returning home with them. Other hospitals prohibited the use of telephone interviews with family members unless a face-to-face meeting was impossible. At another hospital corrective measures were put in place to ensure that all team members had ready access to relevant information when it was found that the social worker had held an in-person meeting with an individual's family and had written a comprehensive note that included information relevant to the discharge plan. That note, however, was put in a bin for filing and did not appear in the record until after the individual had been discharged and had died by suicide. Social workers now file their notes as soon as they are completed. Improving effective communication skills was also the goal of recommendations for role-play training to increase the proficiency of receptionists, switchboard operators, security and other non-clinical staff in gathering information from families.
The need for better communication with other providers of service, including the referring program, was identified at a frequency second only to the need to communicate effectively with families. Past suicide attempts, family member suicides, and persistent suicidal ideation went unreported because of these omissions. As noted earlier, some clinicians did not review treatment records from their very own facility. Tragedy ensued when a clinician did not speak with a private physician who was treating an individual and prescribing medication for chronic pain and in another instance when a substance abuse treatment provider were not contacted. One hospital identified the need to coordinate its own medical, detox and psychiatric services, and cited this as an area for improvement.
Risk /Suicide Assessments
While not negating the responsibility to perform a thorough psychiatric assessment, the need to introduce or revise a formalized, structured lethality assessment was identified in many of the root cause analyses completed following a suicide within three days of discharge. One hospital identified as factors to be considered- history of suicide attempts, risk factors, stressors, access to weapons/means, collateral information, and consultations with other providers. Frequently, the recommendation to develop or revise a risk assessment included the need for a policy that specified the circumstances and frequency with which the assessments must be completed. Specifically, several hospitals identified the need for a documented assessment immediately prior to discharge or when there is any decrease in supervision status.
One hospital in the study now requires that the Director of Inpatient Psychiatry review all individuals admitted on 1:1 supervision and determine when to reduce the observation level. Another hospital changed policy to direct that only physicians may conduct lethality assessments. Hospitals' action plans typically provided for staff training in the use of the assessment tool and monitoring the quality of the tools for a specific period of time.
Falling under the heading of self-evident recommendations, one hospital made procedural changes that require a full team review of all high-risk individuals considered for discharge with a stay of less than seven days. Another hospital instituted a policy requiring a minimum 48-hour stay for individuals with "suicidal ideation, a plan and means." Yet another hospital questioned whether the short length of stay of the decedent had provided sufficient time to accurately judge the effectiveness of treatment.
Treatment Issues
Several of the suicides studied identified opportunities for improvements in treatment which resulted in changes in treatment policies and practices. These addressed:
- securing and reviewing serum levels during rapid medication titration;
- medication trials of sufficient length to ensure clinicians could reliably judge the effectiveness of an anti-depressant medication before changing to another;
- establishing a standard of care for persons diagnosed with depression;
- instituting a benzodiazapine detoxification protocol;
- guidelines for doing urine drug screens;
- expectations around the documentation of the effect of PRN medications in the clinical record;
- tighter supervision of resident physicians' prescribing practices particularly during the first month of rotation;
- expectations around the timeliness and content of discharge notes by social workers and psychiatrists;
- clinical training for staff in therapeutic interventions using role playing and other active teaching techniques;
- changes in the CPEP discharge form to include documentation of health teaching and follow-up appointments; and,
- back-up review of physician discharge medication orders to ensure they are complete.
The inability to form a bond with persons of a different culture and lack of appreciation of the mores of a particular culture were cited in the suicides of two persons of Asian and Middle Eastern descent. In one instance, the facility acknowledged that arranging for interpreter services during therapy sessions was not sufficient to break the isolation of the individual and permit staff to form a bond with him. In another instance, clinical staff did not appreciate the impact of a young person's reconnection with his Middle Eastern heritage and the change this engendered in the way he viewed those closest to him.
The inadvisability of Friday discharges and the lack of acceptable housing options figured in several causal analyses. One root cause analysis characterized shelter housing as disheartening to individuals and as having an undermining effect on all other components of the discharge plan. The need to remain in the hospital because the search for appropriate housing was taking too long led one man to leave the hospital against medical advice, and he died by suicide soon after.
Conclusion
When this report serves as a catalyst for discussion of interventions to reduce suicide risk and resolution to take all steps possible to identify and support persons at risk of suicide, it will have met its objective. The findings from this review support unequivocally the conclusion that comprehensive, thoughtful clinical risk assessments founded on current, accurate and complete information from the individual, family members, past clinical records, and other treatment providers, repeated when clinically indicated and prior to key decisions, remains the strongest single tool in reducing the tragedy of SE suicides.
- AAS Guidelines Help Identify Risk of Suicide for Inpatient and Residential Patients
- J. Knoll, MD: Correctional Suicide Risk Assessment and Prevention. Correctional Mental Health Report, January/February 09.
- S. Shea, MD: The Delicate Art of Eliciting Suicidal Ideation. Psychiatric Annals, May 2004.
- S. Shea, MD: The Delicate Art of Eliciting Suicidal Ideation. Psychiatric Annals, May 2004.
- Suicide in the U.S.: Statistics and Prevention, revised.